Can pulpotomy be the future of tooth preservation? Networks dentists weigh in
Clinical management of irreversible pulpitis
Joana Cunha-Cruz and Thibault Colloc
Collaborators: Janet Clarkson, Craig Ramsay, Ashraf Fouad
Introduction
The standard treatment recommended for permanent teeth that are restorable but have irreversible pulpitis, is conventional root canal treatment. Emerging evidence from randomized controlled trials suggest that pulpotomy with tricalcium silicate-based cements could be a successful alternative intervention, that is less complex and costly. This technique consists of removing coronal pulp to the level of the canal orifices and achieving hemostasis before placing a tricalcium silicate-based cement such as MTA or BiodentineTM in the pulp chamber followed by a definitive restoration.
We asked members of the National Dental Practice-Based Research Network about their experiences to gain an understanding of the current management of irreversible pulpitis in primary care setting in the USA and their views on possible alternative treatment options.
Methods
Study Design and Participants
This is a cross-sectional survey with dental practitioners, members of the National Dental Practice-Based Research Network in the United States.
Data collection
Members of the network were invited to participate in an online survey through email and social media channels. Two email invitations were sent: one in the network’s monthly newsletter sent on May 31, 2022 to all members and one as a follow-up email sent on June 16, 2022 to a targeted audience of members who are general dentists or endodontists. The Quick Poll was announced on the network’s social media accounts (Twitter, Facebook and Instagram). For the first email invitation, approximately 40% of members opened the email and 4% clicked in the survey link. For the targeted email, 46% of members opened the email and 12% clicked the survey link. For social media, six individuals completed the survey. The Quick Poll was open from May 27 until July 5th, 2022. The survey page was opened 1270 times, and 422 individuals submitted survey responses.
Measures and Data Analysis
The survey content included a description of a clinical scenario of a patient with shooting diffuse pain in the lower left quadrant of the mouth that upon examination revealed a carious lesion reaching the pulp of a first permanent molar with no apical radiolucency (Figure 1). The final diagnosis was an irreversible pulpitis with normal apical tissues.
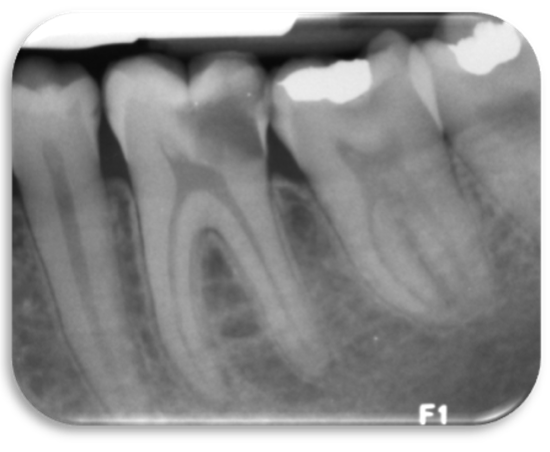
Figure 1. Radiography of a permanent first molar with deep caries used for the clinical scenario
The dental practitioners were asked five questions about their experience dealing with such cases. They were asked how many patients they diagnose with irreversible pulpitis in a month, their most common clinical management strategy used, the number of appointments for a root canal treatment, the material used for pulpotomy (if performed), and if they or their patients would accept a pulpotomy as a definitive treatment.
The data were collected through a web survey in Constant Contact, a digital and email marketing platform. Data were analyzed using descriptive statistics in Stata/SE 17.
Results
Of the 422 dental practitioners who answered the Quick Poll, six were excluded from further analysis because they do not diagnose pulpitis in their practice. The final sample size was 416 and 52% diagnosed irreversible pulpitis in 1 to 5 patients per month, 25% in 6 to 10 patients, and 23% in 10 or more patients (Table 1, and Figure 2).
As expected, the vast majority of practitioners selected root canal therapy (n=319, 77%) as a common strategy for the management of irreversible pulpitis, with about half of them selecting it as the single most common strategy (n=180, 43%). Root canal therapy on a molar tooth is most performed in two appointments (31%), or a single appointment (22%), with a few doing it in three appointments (3%). Interestingly, 32% of respondents would refer the patient in the clinical scenario to a specialist, and 12% of respondents do not perform root canal treatments on any teeth.
When queried about their most common strategies for the management of irreversible pulpitis, 58% of the respondents selected one strategy, 24% two strategies and 18% three or more strategies. After root canal therapy, analgesic prescription or recommendation was the second most common strategy (30%), followed by the other three strategies, all with approximately 20% of practitioners. Thus, one fifth of practitioners (n=83, 20%) included pulpotomy as one of the most common clinical management strategies for irreversible pulpitis with normal apical tissues.
Approximately half of the practitioners used pulpotomy as part of their practice (55%, n=230). Among them, the most common materials used for pulpotomies were calcium hydroxide (44%), and Mineral Trioxide Aggregate (MTA) (24%), followed by the other four materials (formocreosol, glass ionomer, zinc oxide cement, and other tricalcium silicate-based cements), all with approximately 20% of practitioners. Thus, among all respondents of the survey, pulpotomy with tricalcium silicate-based cements such as MTA, BiodentineTM and EndoSequence® Root Repair MaterialTM is a treatment option being employed by 19.5% of the practitioners surveyed (n=81).
Almost half of practitioners (44%) felt that both themselves and their patients would be in favor of pulpotomy as a definitive treatment for the management of irreversible pulpitis compared to conventional root canal treatment, assuming that there is sufficient tooth structure and there is no need for post retention of the restoration. Twenty-four percent of the practitioners felt that their patients would be in favor, but not themselves. Only 3% of practitioners felt that they would be in favor, but not their patients. Approximately one third felt neither the patients nor themselves would be in favor (28%). Thus, a total of 47% of practitioners were in favor of pulpotomy as a definitive procedure and 68% of practitioners felt that their patients would be in favor of this procedure.
Highlights
Approximately half of the practitioners used pulpotomy as part of their practice (55%, n=271).
Pulpotomy with tricalcium silicate-based cements such as MTA, BiodentineTM and EndoSequence® Root Repair MaterialTM is a treatment option being employed by 19.5% of the practitioners surveyed (n=81).
47% of practitioners were in favor of pulpotomy as a definitive procedure and 68% of practitioners felt that their patients would be in favor of this procedure.
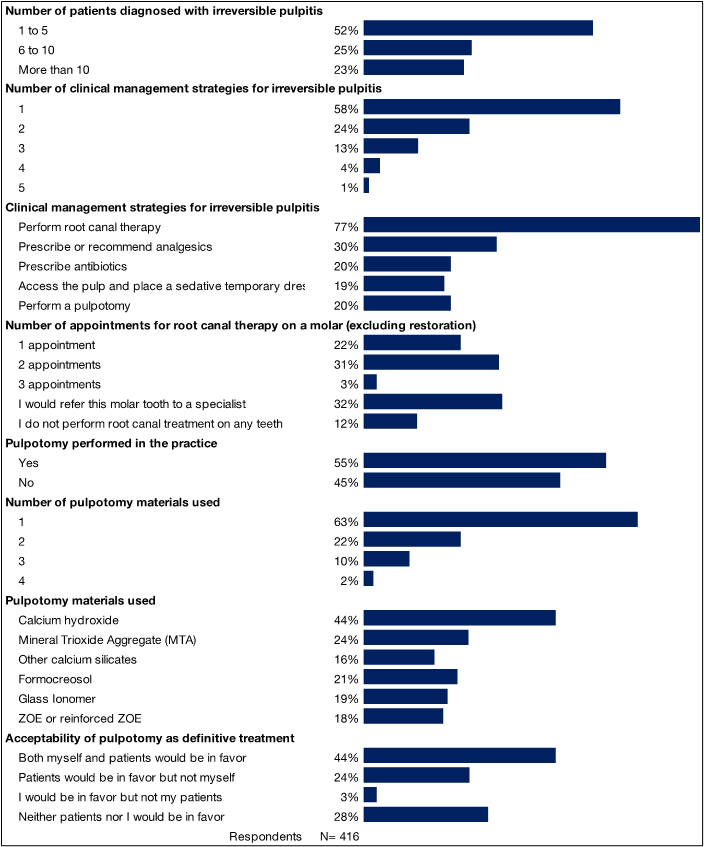
Table 1. Experience of dental practitioners with the management of irreversible pulpitis: National Dental Practice-Based Research, 2022.
| N N=416 |
% | ||
| Number of patients diagnosed with irreversible pulpitis | |||
| 1 to 5 | 218 | 52% | |
| 6 to 10 | 103 | 25% | |
| More than 10 | 95 | 23% | |
| Number of clinical management strategies for irreversible pulpitis | |||
| 1 | 243 | 58% | |
| 2 | 100 | 24% | |
| 3 | 52 | 13% | |
| 4 | 16 | 4% | |
| 5 | 5 | 1% | |
| Clinical management strategies for irreversible pulpitis | |||
| Perform root canal therapy | 319 | 77% | |
| Prescribe or recommend analgesics | 126 | 30% | |
| Prescribe antibiotics | 83 | 20% | |
| Access the pulp and place a sedative temporary dressing | 77 | 19% | |
| Perform a pulpotomy | 83 | 20% | |
| Number of appointments for root canal therapy on a molar (excluding restoration) | |||
| 1 appointment | 92 | 22% | |
| 2 appointments | 128 | 31% | |
| 3 appointments | 12 | 3% | |
| I would refer this molar tooth to a specialist | 132 | 32% | |
| I do not perform root canal treatment on any teeth | 51 | 12% | |
| Pulpotomy performed in the practice | |||
| Yes | 230 | 55% | |
| No | 186 | 45% | |
| Number of pulpotomy materials used | |||
| 1 | 144 | 63% | |
| 2 | 51 | 22% | |
| 3 | 24 | 10% | |
| 4 | 5 | 2% | |
| Pulpotomy materials used | |||
| Calcium hydroxide | 101 | 44% | |
| Mineral Trioxide Aggregate (MTA) | 55 | 24% | |
| Other calcium silicates | 37 | 16% | |
| Formocreosol | 49 | 21% | |
| Glass Ionomer | 44 | 19% | |
| ZOE or reinforced ZOE | 42 | 18% | |
| Acceptability of pulpotomy as definitive treatment | |||
| Both myself and patients would be in favor | 182 | 44% | |
| Patients would be in favor but not myself | 100 | 24% | |
| I would be in favor but not my patients | 12 | 3% | |
| Neither patients nor I would be in favor | 118 | 28% | |
Figure 2. Experience of dental practitioners with the management of irreversible pulpitis: National Dental Practice-Based Research, 2022.
Interested in Becoming a Member?
Related Posts


