Deep Margin Elevation Quick Poll Results
Highlights
- About half of the 533 respondents (52%) were familiar with the Deep Margin Elevation technique and 148 had used it (28%).
- Most practitioners would restore function by placing a “Core + Full Crown or Onlay” (63%)
- Practitioners were evenly split concerning the clinical indication/use of crown lengthening and about one-third (35%) would do root canal therapy.
Authors
Saulo Geraldeli, DDS, MS, PhD, East Carolina University School of Dental Medicine, Greenville, NC
Mark E Moss, DDS, PhD, East Carolina University School of Dental Medicine. Greenville, NC
Introduction and Methods
The deep margin elevation (DME) is a less-expensive, less-invasive technique proposed in 19982 indicated for tooth preparations of semi-direct and indirect adhesive restorations when the gingival margins cannot be isolated with rubber dam alone. However, there is no information as to how this technique is recommended by general practitioners in the USA. Therefore, a 5-question Quick Poll on indications for DME was conducted by the National Dental Practice-based Research Network.
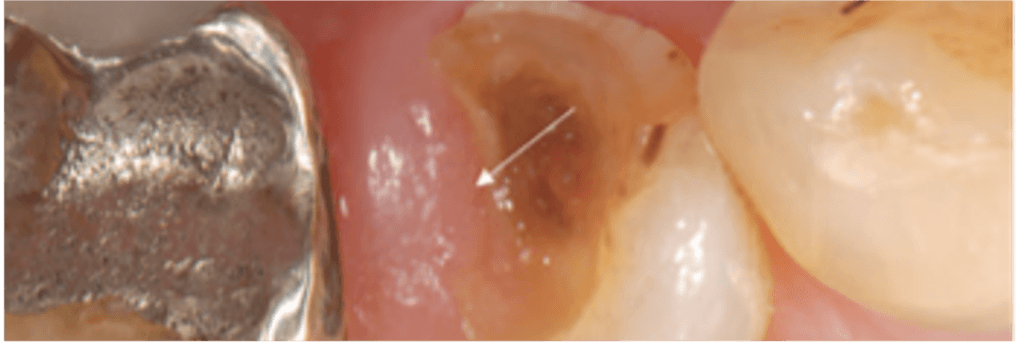
A cross-sectional survey with dental practitioners, members of the National Dental Practice-Based Research Network in the United States included a clinical scenario, with a radiograph and a photograph from a published study1 (Figure 1, used with permission1). Members of the network were invited to participate via email and the survey was open from Nov 18 until Dec 17, 2021. The data were collected through a web survey in Constant Contact, a digital and email marketing platform. Data were analyzed using descriptive statistics.
The case was described as follows: “An adult patient presents with restoration loss on the mandibular right premolar. Upon clinical and radiographic examination, you diagnose superficial demineralized dentin reaching beyond the CEJ with the proximal margin partially covered by overgrowing gingival tissue. The tooth is vital and there is no periapical radiolucency. What would be your most likely standard of care treatment approach for this case scenario in your practice?”
Specific questions were:
- Would you do crown lengthening?
- Would you do root canal therapy?
- How would you restore function?
- How often do patients in your practice in a similar situation decide to extract the tooth rather than restore it?
The final question asked whether the dentist was familiar with a technique referred to as Deep Margin Elevation (DME), Coronal Margin Relocation (CMR), or Proximal Box Elevation (PBE).
Results
There were 533 responses. The respondents were evenly split concerning the clinical indication/use of crown lengthening, with 48% stating that they would do crown lengthening to address this clinical scenario. About one-third (35%) would do root canal therapy.
Table 1. – Number and percentage of responses for specific questions
| Yes | No | Total | |
| Would you do crown lengthening? | 257 (48.2%) | 276 (51.8%) | 533 (100%) |
| Would you do RCT? | 184 (34.5%) | 349 (65.5%) | 533 (100%) |
The responses for the clinical options to restore function are shown in Figure 1. Most practitioners chose “Core build up + Full Crown or Onlay” (63%). Only 1% would restore with amalgam.

Among the respondents, only about 10% reported a high likelihood that patients in their practice would decide to have the tooth extracted. Most (44%) felt that less than 25% of the patients in their practice would opt for an extraction when a scenario similar to this clinical situation arose (Figure 2).

About half of the 533 respondents (48%) were not familiar with the technique described as DME (Table 2). However, among the 279 who had heard of it, 148 (53%) had used it.
Table 2. Percentage of respondents with awareness of the DME technique
| Not heard of DME | Have heard of DME but have not used | Yes, have used DME | Total | |
| Prior to today, had you been aware of this restorative dentistry technique? | 254 (47.7%) | 131 (24.6%) | 148 (27.8%) | 533 (100%) |
Further analysis showed that practitioners who have heard of the DME technique but have not used it were more likely to state that their practice had a higher proportion of patients who would opt for extraction relative to the dentists who have used DME, and dentists who had not heard of DME (Figure 3; Chi square test, p=0.03).

Conclusion
Most practitioners restore function of teeth with deep proximal caries partially covered by gingival tissue using a core build up and a full crown or onlay. Many practitioners have heard of the deep margin elevation technique, a less expensive and invasive technique, and a third used it to treat their patients.
References
1 Frese, C., Wolff, D. & Staehle, H. J. Proximal box elevation with resin composite and the dogma of biological width: clinical R2-technique and critical review. Oper Dent 39, 22-31, doi:10.2341/13-052-T (2014).
2 Dietschi, D. & Spreafico, R. Current clinical concepts for adhesive cementation of tooth-colored posterior restorations. Pract Periodontics Aesthet Dent 10, 47-54; quiz 56 (1998).
* Pictures used by permission from Frese et al. Proximal box elevation with resin composite and the dogma of biological width: clinical R2-technique and critical review Oper Dent 39, 22-31. © Operative Dentistry, Inc. Transmission or reproduction of protected items beyond that allowed by fair use requires the written permission of Operative Dentistry, Inc.
Interested in Becoming a Member?
Related Posts


